


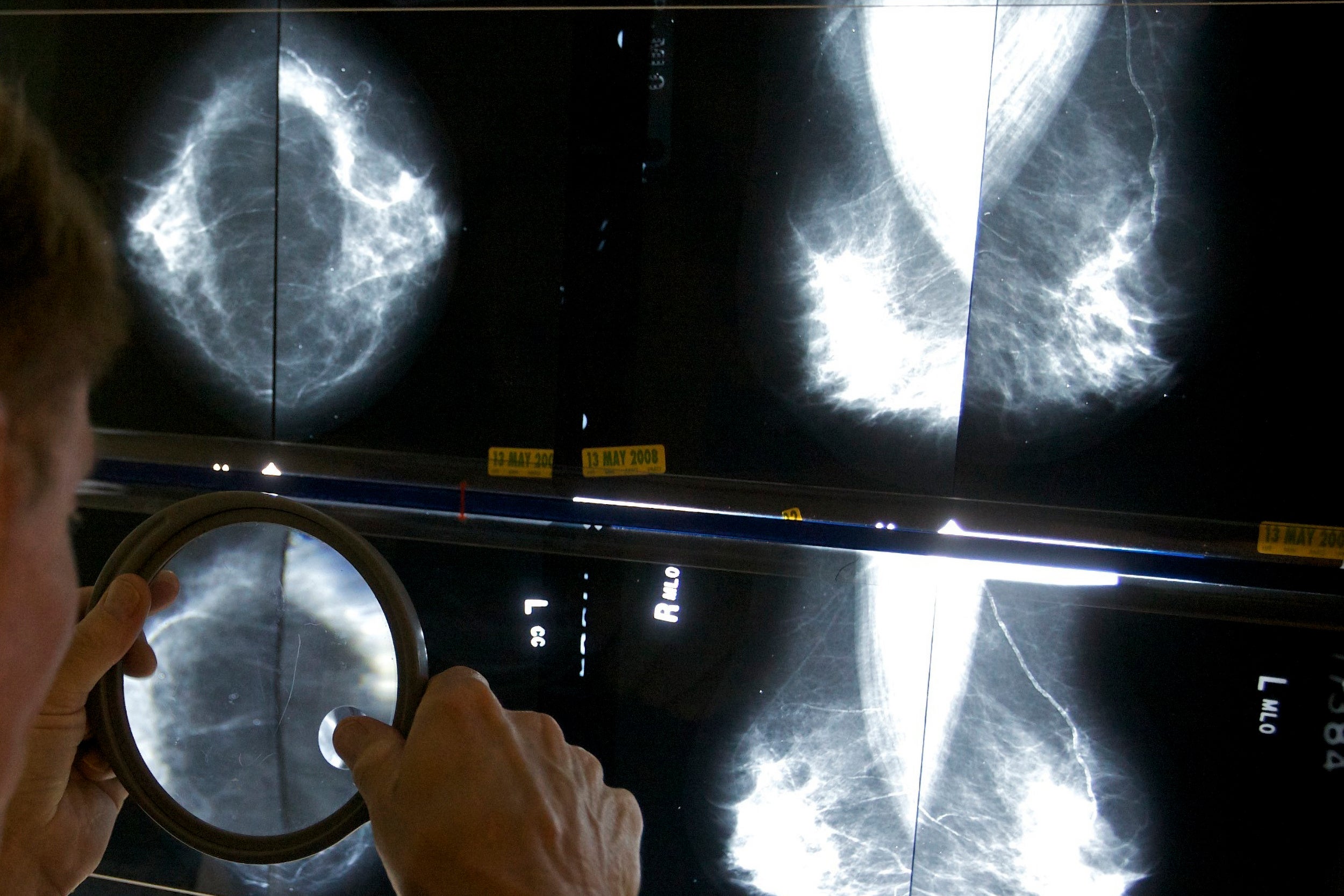
AP Photo
Health
Why are ineffective oral decongestants still on store shelves?
Drug regulation expert explains how problem was discovered, next steps for FDA, questions it raises about other products, supplements
A Food and Drug Administration advisory panel concluded last week that the decongestant phenylephrine, contained in many over-the-counter cold remedies — including some formulations of popular brands like Sudafed, Tylenol, and Nyquil — is ineffective when taken orally. The finding potentially upsets a significant part of the over-the-counter market for cold and flu remedies as summer fades, and the cold and flu season approaches.
The Gazette spoke with Aaron Kesselheim, a professor of medicine at Harvard Medical School and at Brigham and Women’s Hospital. Kesselheim, who leads Brigham’s Program on Regulation, Therapeutics, and Law and is a member of the HMS Center for Bioethics, explains why it took so long for the FDA to act and why it might be a while before the drugs disappear from pharmacy shelves. This interview was edited for length and clarity.
Q&A: Aaron Kesselheim
GAZETTE: Does this decision have some roots in the methamphetamine epidemic?
KESSELHEIM: In an indirect way, yes. For a long time, over-the-counter decongestant products like Sudafed had pseudoephedrine in them. Pseudoephedrine is effective at reducing sinus congestion during colds but is also an ingredient that can be used to make methamphetamine. As a result of abuse of pseudoephedrine-containing products by manufacturers of methamphetamine, federal legislation was passed moving those products behind the pharmacy counter, which made them harder for people to get ahold of for routine use. Since companies would prefer to sell products that people can just easily grab off the shelves, Sudafed and other well-known brands introduced new formulations with another very old over-the-counter active ingredient, phenylephrine. The problem is that phenylephrine doesn’t work, as the FDA finally concluded, unless you directly spritz it onto your nasal passages as with Afrin or products like that.

“Part of the problem is that phenylephrine is a very old product, so old in fact that when it reached the market, it did so without the sort of evidence we would expect today from new drug approvals,” said Aaron Kesselheim.
Kris Snibbe/Harvard Staff Photographer
GAZETTE: How does something ineffective in many formulations become so widespread? Companies must have known.
KESSELHEIM: Part of the problem is that phenylephrine is a very old product, so old in fact that when it reached the market, it did so without the sort of evidence we would expect today from new drug approvals. It predates the congressional Kefauver Harris Amendments of 1962 that required drugs to be proven to be effective before they could be sold.
After 1962 the FDA engaged in a multidecade process of reviewing thousands of medications that had been approved between 1938 and 1962 to determine they worked. But there were tens of thousands of over-the-counter drugs like phenylephrine, so the FDA said, “Given the fact that there are so many of these, it would be impractical to review them individually,” as they were mostly doing for prescription drugs.
Instead, when it came time to review the OTC products starting in the 1970s, they created large groupings of over-the-counter products under what they called “monographs” and made judgments on them through a rule-making process.
Phenylephrine was validated under the monograph process, although the data on which the judgment was based was not very rigorous. But making changes to the monograph system was really resource- and time-intensive, so OTC drugs like phenylephrine could persist on the market even as evidence accumulated that they did not actually work as expected.
GAZETTE: But in the meantime, phenylephrine has become very common as an oral decongestant?
KESSELHEIM: That’s right. With the transfer to behind the counter of a lot of pseudoephedrine products, manufacturers had brands that they were trying to maintain, like Sudafed, and were looking for other active ingredients to put in their product. Since phenylephrine was included in the OTC decongestant monograph, they still sell OTC Sudafed and legitimately say, “We’ve got a decongestant in our product.” The problem is that there was a growing body of evidence that phenylephrine did not work as a decongestant when administered orally.
GAZETTE: From a consumer point of view, phenylephrine is safe, so people shouldn’t worry if they’ve taken it or have it in their medicine cabinet?
KESSELHEIM: That’s right. It is just ineffective.
GAZETTE: This was an advisory panel. What happens next?
KESSELHEIM: If the FDA decides it agrees with the unanimous vote that the drug doesn’t work, it has to go through an administrative process to change the monograph and formally withdraw phenylephrine from the market.
Since there does not appear to be an imminent safety risk, the FDA cannot use any emergency powers to pull the product off the market. If the FDA removes phenylephrine from the OTC decongestant monograph, then any product that has phenylephrine in it and claims that it’s a decongestant is misbranded and would have to be removed from the market. Meanwhile, manufacturers can take proactive steps to reformulate their products.
“Since there does not appear to be an imminent safety risk, the FDA cannot use any emergency powers to pull the product off the market.”
GAZETTE: And the exception here, as you pointed out, are nasal sprays where it actually does work as a decongestant?
KESSELHEIM: Yes, that is something that may cause confusion from a patient point of view, if the main message that is getting through is “this drug doesn’t work.” But if you administer it directly to the nasal passages there is evidence that it works. It doesn’t work if it’s ingested, as in a pill form.
More like this


GAZETTE: Is there any doubt that the FDA will follow its advisory panel’s finding?
KESSELHEIM: I was on the Advisory Committee that reviewed the controversial Alzheimer’s drug aducanumab in 2020. After we gave it a near-unanimous negative vote, the FDA did not follow our advice. We said FDA shouldn’t approve the drug, and it was approved anyway. [Kesselheim resigned from that committee as a result of the decision.] But generally, according to a study recently published by my colleague Joseph Daval, [a research fellow in medicine] in my research group, FDA follows the advice of its advisory committees about 80 percent of the time.
GAZETTE: It sounds like this process will take months to work out.
KESSELHEIM: Months would be shockingly fast. When the FDA took steps to remove ephedrine from OTC dietary supplements — a product that was legitimately dangerous — it took years to take it through the administrative process. If the FDA declares that it favors removing the drug from the market, and manufacturers do not voluntarily comply such that FDA has to go through the full rule-making process, it could actually take quite a long time.
GAZETTE: Do you expect manufacturers to comply?
KESSELHEIM: I expect some manufacturers to comply, but I do not expect all of them to comply. The easiest way to continue to make money is to continue to sell the product in its current formulation until you’re required to take it off the market. And if there’s no imminent safety issue, manufacturers aren’t going to have a lot of pressure from mounting drug risks to pull the product off market or reformulate their products.
GAZETTE: How should consumers think about this? Has trust with these manufacturers been broken here, or are people already jaded about these products?
KESSELHEIM: I think the trust issue is an important one. This sheds light on the fact that there are a lot of products being sold at your local pharmacy or grocery store that don’t have the same level of evidence behind them that we expect from prescription medications. In this case it was for historical reasons, but there are other cases, like nutritional supplements that don’t work and are still sold with health-supporting claims because such supplements were statutorily excluded from FDA oversight by the DSHEA Act (Dietary Supplement Health and Education Act of 1994).
So, one of the lessons for consumers is that it’s important to talk about these products with your health professional before you use them. It also speaks to the important role that the FDA plays in helping decide where the evidence is strong and where the evidence is weak around those products.
There are a lot of people out there who would try to take the FDA out of its oversight role, which would be a bad thing to do. Reducing the FDA’s power to approve effective and safe products would move us back to a pre-1962 market when lots of drugs like phenylephrine were being sold. This is a good example of why it’s important to have an expert regulatory body to adjudicate the evidence behind the products that we use.